Types of Diabetes
The 3 main types of
diabetes are type 1, type 2 & gestational diabetes.
- Type 1 diabetes, formerly
called juvenile diabetes, is usually first diagnosed in children, teenagers, or young adults.
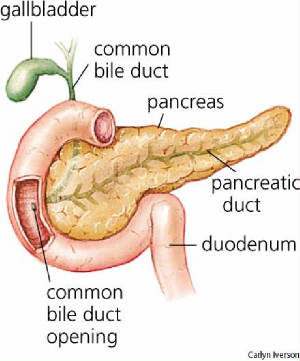
In this form of diabetes, the beta cells of the pancreas no longer make insulin because the body's immune system has attacked & destroyed them.
- Type 2 diabetes, formerly
called adult-onset diabetes, is the most common form. People can develop it at any age,
even during childhood. This form of diabetes usually begins with insulin resistance, a condition
in which muscle, liver & fat cells don't use insulin properly.
At first,
the pancreas keeps up with the added demand by producing more insulin. In time, however,
it loses the ability to secrete enough insulin in response to meals.
- Gestational diabetes develops
in some women during the late stages of pregnancy. Although this form of diabetes usually
goes away after the baby is born, a woman who has had it is more likely to develop type 2 diabetes
later in life. Gestational diabetes is caused by the hormones of pregnancy or by a shortage
of insulin.
Type 1 Diabetes & Type 2 Diabetes
To move away from basing the names of the 2 main types of diabetes on treatment or age at onset,
an American Diabetes Association expert committee recommended in 1997 universal adoption of simplified terminology. The National
Institute of Diabetes & Digestive & Kidney Diseases (NIDDK) agrees.
|
Former Names |
Preferred Names |
Type I
juvenile diabetes
insulin-dependent diabetes mellitus
IDDM |
type 1 diabetes |
Type II
adult-onset diabetes
noninsulin-dependent diabetes mellitus
NIDDM |
type 2 diabetes |
What is pre-diabetes?
In pre-diabetes, blood glucose
levels are higher than normal but not high enough to be characterized as diabetes. However,
many people with pre-diabetes develop type 2 diabetes
within 10 years. Pre-diabetes also increases the risk of heart disease & stroke.
With modest weight loss & moderate physical activity,
people with pre-diabetes can delay or prevent type 2 diabetes.
How are diabetes & pre-diabetes diagnosed?
The following tests are used for diagnosis:
- A fasting plasma glucose test
measures your blood glucose after you have gone at least 8 hours without eating. This test is used to detect diabetes or pre-diabetes.
- An oral glucose tolerance test
measures your blood glucose after you have gone at least 8 hours without eating and 2 hours after you drink a glucose-containing
beverage. This test can be used to diagnose diabetes or pre-diabetes.
- In a random plasma glucose test,
your doctor checks your blood glucose without regard to when you ate your last meal. This test, along with an assessment of
symptoms, is used to diagnose diabetes but not pre-diabetes.
Positive test results should
be confirmed by repeating the fasting plasma glucose test or the oral glucose tolerance test on a different day.
Fasting Plasma Glucose (FPG) Test
The FPG is the preferred test for diagnosing
diabetes due to convenience & is most reliable when done in the morning.
Results & their meaning are shown in table 1. If your
fasting glucose level is 100 to 125 mg/dL, you have a form of pre-diabetes called impaired fasting glucose (IFG), meaning
that you're more likely to develop type 2 diabetes but don't have it yet.
A level of 126 mg/dL or above, confirmed by repeating the
test on another day, means that you have diabetes.
Table 1. Fasting Plasma Glucose Test
| Plasma Glucose Result (mg/dL) |
Diagnosis |
| 99 & below |
Normal |
| 100 to 125 |
Pre-diabetes
(impaired fasting glucose) |
| 126 & above |
Diabetes* |
*Confirmed by repeating the test on a different day.
Oral Glucose Tolerance Test (OGTT)
Research has shown that the OGTT is more sensitive than the
FPG test for diagnosing pre-diabetes, but it's less convenient to administer.
The OGTT requires you to fast for at least 8 hours before the test. Your plasma glucose is measured
immediately before & 2 hours after you drink a liquid containing 75 grams of glucose dissolved in water.
Results & what they mean are shown in table 2.
If your blood glucose level is between 140 & 199 mg/dL 2 hours after drinking the liquid,
you have a form of pre-diabetes called impaired glucose tolerance or IGT, meaning that you're more likely to develop type
2 diabetes but don't have it yet.
A 2-hour glucose level of 200 mg/dL or above, confirmed by repeating the test on another day,
means that you have diabetes.
Table 2. Oral Glucose Tolerance Test
| 2-Hour Plasma Glucose Result (mg/dL) |
Diagnosis |
| 139 & below |
Normal |
| 140 to 199 |
Pre-diabetes
(impaired glucose tolerance) |
| 200 & above |
Diabetes* |
*Confirmed by repeating the test on a different day.
Gestational diabetes is also diagnosed based on plasma glucose
values measured during the OGTT.
Blood glucose levels are checked 4 times during the test.
If your blood glucose levels are above normal at least twice during the test, you have gestational diabetes.
Table 3 shows the above-normal results for the OGTT for gestational
diabetes.
Table 3. Gestational Diabetes: Above-Normal
Results for the Oral Glucose Tolerance Test
| When |
Plasma Glucose Result (mg/dL) |
| Fasting |
95 or higher |
| At 1 hour |
180 or higher |
| At 2 hours |
155 or higher |
| At 3 hours |
140 or higher |
Note: Some laboratories use other numbers for this test.
For additional information about the diagnosis and treatment of gestational diabetes, see the NIDDK
booklet What I Need to Know About Gestational Diabetes.
Random Plasma Glucose Test
A random blood glucose level of 200 mg/dL or more, plus presence
of the following symptoms, can mean that you have diabetes:
- increased urination
- increased thirst
- unexplained weight loss
Other symptoms include:
- fatigue
- blurred vision
- increased hunger
- sores that don't heal
Your doctor will check your blood glucose level on another day
using the FPG or the OGTT to confirm the diagnosis.
What factors increase my risk for type 2 diabetes?
To find out your risk, check each item that applies to you.
- I am 45 or older.
- I am overweight or obese (see the body mass index [BMI] in table 4).
- I have a parent, brother, or sister with diabetes.
- My family background is African American, American Indian, Asian American, Pacific Islander,
or Hispanic American/Latino.
- I have had gestational diabetes, or I gave birth to at least one baby weighing more than 9
pounds.
- My blood pressure is 140/90 or higher, or I have been told that I have high blood pressure.
- My cholesterol levels are not normal. My HDL cholesterol ("good" cholesterol) is 35 or lower,
or my triglyceride level is 250 or higher.
- I am fairly inactive. I exercise fewer than three times a week.
Checking My Weight
BMI is a measure used to evaluate body weight relative to height.
You can use BMI to find out whether you are underweight, normal weight, overweight, or obese. Use table 4 to find your BMI.
- Find your height in the left-hand column.
- Move across in the same row to the number closest to your weight.
The number at the top of that column is your BMI. Check the word above your BMI to see whether
you are normal weight, overweight, or obese. If you are overweight or obese, talk with your doctor about ways to lose weight
to reduce your risk of diabetes or pre-diabetes.
Table 4. Body Mass Index
| |
Normal |
Overweight |
Obese |
| BMI |
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
32 |
33 |
34 |
35 |
36 |
Height
(inches) |
Body Weight (pounds) |
| 58 |
91 |
96 |
100 |
105 |
110 |
115 |
119 |
124 |
129 |
134 |
138 |
143 |
148 |
153 |
158 |
162 |
167 |
172 |
| 59 |
94 |
99 |
104 |
109 |
114 |
119 |
124 |
128 |
133 |
138 |
143 |
148 |
153 |
158 |
163 |
168 |
173 |
178 |
| 60 |
97 |
102 |
107 |
112 |
118 |
123 |
128 |
133 |
138 |
143 |
148 |
153 |
158 |
163 |
168 |
174 |
179 |
184 |
| 61 |
100 |
106 |
111 |
116 |
122 |
127 |
132 |
137 |
143 |
148 |
153 |
158 |
164 |
169 |
174 |
180 |
185 |
190 |
| 62 |
104 |
109 |
115 |
120 |
126 |
131 |
136 |
142 |
147 |
153 |
158 |
164 |
169 |
175 |
180 |
186 |
191 |
196 |
| 63 |
107 |
113 |
118 |
124 |
130 |
135 |
141 |
146 |
152 |
158 |
163 |
169 |
175 |
180 |
186 |
191 |
197 |
203 |
| 64 |
110 |
116 |
122 |
128 |
134 |
140 |
145 |
151 |
157 |
163 |
169 |
174 |
180 |
186 |
192 |
197 |
204 |
209 |
| 65 |
114 |
120 |
126 |
132 |
138 |
144 |
150 |
156 |
162 |
168 |
174 |
180 |
186 |
192 |
198 |
204 |
210 |
216 |
| 66 |
118 |
124 |
130 |
136 |
142 |
148 |
155 |
161 |
167 |
173 |
179 |
186 |
192 |
198 |
204 |
210 |
216 |
223 |
| 67 |
121 |
127 |
134 |
140 |
146 |
153 |
159 |
166 |
172 |
178 |
185 |
191 |
198 |
204 |
211 |
217 |
223 |
230 |
| 68 |
125 |
131 |
138 |
144 |
151 |
158 |
164 |
171 |
177 |
184 |
190 |
197 |
203 |
210 |
216 |
223 |
230 |
236 |
| 69 |
128 |
135 |
142 |
149 |
155 |
162 |
169 |
176 |
182 |
189 |
196 |
203 |
209 |
216 |
223 |
230 |
236 |
243 |
| 70 |
132 |
139 |
146 |
153 |
160 |
167 |
174 |
181 |
188 |
195 |
202 |
209 |
216 |
222 |
229 |
236 |
243 |
250 |
| 71 |
136 |
143 |
150 |
157 |
165 |
172 |
179 |
186 |
193 |
200 |
208 |
215 |
222 |
229 |
236 |
243 |
250 |
257 |
| 72 |
140 |
147 |
154 |
162 |
169 |
177 |
184 |
191 |
199 |
206 |
213 |
221 |
228 |
235 |
242 |
250 |
258 |
265 |
| 73 |
144 |
151 |
159 |
166 |
174 |
182 |
189 |
197 |
204 |
212 |
219 |
227 |
235 |
242 |
250 |
257 |
265 |
272 |
| 74 |
148 |
155 |
163 |
171 |
179 |
186 |
194 |
202 |
210 |
218 |
225 |
233 |
241 |
249 |
256 |
264 |
272 |
280 |
| 75 |
152 |
160 |
168 |
176 |
184 |
192 |
200 |
208 |
216 |
224 |
232 |
240 |
248 |
256 |
264 |
272 |
279 |
287 |
| 76 |
156 |
164 |
172 |
180 |
189 |
197 |
205 |
213 |
221 |
230 |
238 |
246 |
254 |
263 |
271 |
279 |
287 |
295 |
| |
Obese |
Extreme Obesity |
| BMI |
37 |
38 |
39 |
40 |
41 |
42 |
43 |
44 |
45 |
46 |
47 |
48 |
49 |
50 |
51 |
52 |
53 |
54 |
Height
(inches) |
Body Weight (pounds) |
| 58 |
177 |
181 |
186 |
191 |
196 |
201 |
205 |
210 |
215 |
220 |
224 |
229 |
234 |
239 |
244 |
248 |
253 |
258 |
| 59 |
183 |
188 |
193 |
198 |
203 |
208 |
212 |
217 |
222 |
227 |
232 |
237 |
242 |
247 |
252 |
257 |
262 |
267 |
| 60 |
189 |
194 |
199 |
204 |
209 |
215 |
220 |
225 |
230 |
235 |
240 |
245 |
250 |
255 |
261 |
266 |
271 |
276 |
| 61 |
195 |
201 |
206 |
211 |
217 |
222 |
227 |
232 |
238 |
243 |
248 |
254 |
259 |
264 |
269 |
275 |
280 |
285 |
| 62 |
202 |
207 |
213 |
218 |
224 |
229 |
235 |
240 |
246 |
251 |
256 |
262 |
267 |
273 |
278 |
284 |
289 |
295 |
| 63 |
208 |
214 |
220 |
225 |
231 |
237 |
242 |
248 |
254 |
259 |
265 |
270 |
278 |
282 |
287 |
293 |
299 |
304 |
| 64 |
215 |
221 |
227 |
232 |
238 |
244 |
250 |
256 |
262 |
267 |
273 |
279 |
285 |
291 |
296 |
302 |
308 |
314 |
| 65 |
222 |
228 |
234 |
240 |
246 |
252 |
258 |
264 |
270 |
276 |
282 |
288 |
294 |
300 |
306 |
312 |
318 |
324 |
| 66 |
229 |
235 |
241 |
247 |
253 |
260 |
266 |
272 |
278 |
284 |
291 |
297 |
303 |
309 |
315 |
322 |
328 |
334 |
| 67 |
236 |
242 |
249 |
255 |
261 |
268 |
274 |
280 |
287 |
293 |
299 |
306 |
312 |
319 |
325 |
331 |
338 |
344 |
| 68 |
243 |
249 |
256 |
262 |
269 |
276 |
282 |
289 |
295 |
302 |
308 |
315 |
322 |
328 |
335 |
341 |
348 |
354 |
| 69 |
250 |
257 |
263 |
270 |
277 |
284 |
291 |
297 |
304 |
311 |
318 |
324 |
331 |
338 |
345 |
351 |
358 |
365 |
| 70 |
257 |
264 |
271 |
278 |
285 |
292 |
299 |
306 |
313 |
320 |
327 |
334 |
341 |
348 |
355 |
362 |
369 |
376 |
| 71 |
265 |
272 |
279 |
286 |
293 |
301 |
308 |
315 |
322 |
329 |
338 |
343 |
351 |
358 |
365 |
372 |
379 |
386 |
| 72 |
272 |
279 |
287 |
294 |
302 |
309 |
316 |
324 |
331 |
338 |
346 |
353 |
361 |
368 |
375 |
383 |
390 |
397 |
| 73 |
280 |
288 |
295 |
302 |
310 |
318 |
325 |
333 |
340 |
348 |
355 |
363 |
371 |
378 |
386 |
393 |
401 |
408 |
| 74 |
287 |
295 |
303 |
311 |
319 |
326 |
334 |
342 |
350 |
358 |
365 |
373 |
381 |
389 |
396 |
404 |
412 |
420 |
| 75 |
295 |
303 |
311 |
319 |
327 |
335 |
343 |
351 |
359 |
367 |
375 |
383 |
391 |
399 |
407 |
415 |
423 |
431 |
| 76 |
304 |
312 |
320 |
328 |
336 |
344 |
353 |
361 |
369 |
377 |
385 |
394 |
402 |
410 |
418 |
426 |
435 |
443 |
When should I be tested for diabetes?
Anyone 45 years old or older
should consider getting tested for diabetes. If you're 45 or older & your BMI indicates that you're overweight (see table 4),
it's strongly recommended that you get tested.
If you're younger than 45, are overweight & have 1 or more
of the risk factors, you should consider testing.
Ask your doctor for a FPG or an OGTT. Your doctor will tell
you if you have normal blood glucose, pre-diabetes, or diabetes.
If your blood glucose is higher than normal but lower than the
diabetes range (called pre-diabetes), have your blood glucose checked in 1 to 2 years.
How is diabetes managed?
If you're diagnosed with diabetes, you can manage it with:
- meal planning
- physical activity
- & if needed, medications
Points to Remember
- Diabetes & pre-diabetes are diagnosed by checking blood
glucose levels.
- Many people with pre-diabetes develop type 2 diabetes within
10 years.
- If you have pre-diabetes, you can delay or prevent type 2 diabetes
with a low-fat, low-calorie diet, modest weight loss & regular physical activity.
- If you're 45 or older, you should consider getting tested for
diabetes. If you're 45 or older & overweight, it's strongly recommended that you get tested.
- If you're younger than 45, are overweight & have
1 or more of the risk factors, you should consider testing.
A Fact Sheet
from the National Diabetes Education Program
Type 1 diabetes
in U.S. children & adolescents may be increasing
& many more new cases of type 2 diabetes are being reported in young people.
Standards of care for managing children with
diabetes issued by the American Diabetes Association in January 2005 provide more guidance than previously given.
To update primary care providers & their
staff members on this rapidly changing area of diabetes care, the National Diabetes Education Program (NDEP) has developed
this overview of the current literature.
What Is Diabetes?
Diabetes mellitus is a group of diseases characterized
by high levels of blood glucose resulting from defects in insulin production, insulin action, or both.
Diabetes can be associated with serious complications
& premature death, but people with diabetes can take steps to control the disease & lower the risk of complications.
Type 1 Diabetes
Type 1 diabetes is an autoimmune disease in which
the immune system destroys the insulin-producing beta cells of the pancreas that regulate blood glucose.
Type 1 diabetes has an acute onset, with children
& adolescents usually able to pinpoint when symptoms began. Onset can occur at any age, but it most often occurs in children
& young adults.
Since the pancreas can no longer produce insulin,
people with type 1 diabetes require daily injections of insulin for life. Children with type 1 diabetes are at risk for long-term
complications (damage to cardiovascular system, kidneys, eyes, nerves, blood vessels, gums & teeth).
Type 1 diabetes accounts for 5 to 10% of all diagnosed
cases of diabetes, but is the leading cause of diabetes in children. A diabetes management plan for young people includes
insulin therapy, self-monitoring of blood glucose, healthy eating & physical activity.
The plan is designed to ensure proper growth &
prevention of hypoglycemia. New management strategies are helping children with type 1 diabetes live long & healthy lives.
Symptoms. The
symptoms of type 1 diabetes usually develop over a short period of time.They include:
Children also may feel very tired. If not diagnosed
& treated with insulin, the individual with type 1 diabetes
can lapse into a life-threatening diabetic coma, known as diabetic ketoacidosis or DKA.
Often, children will present with vomiting, a sign
of DKA & mistakenly be diagnosed as having gastroenteritis.
New-onset diabetes can be differentiated from a GI infection
by the frequent urination that accompanies continued vomiting as opposed to decreased urination due to dehydration if the vomiting is caused by a GI “bug.”
Risk Factors. A
combination of genetic & environmental factors put people at increased risk for type 1 diabetes. Researchers are working to identify these factors & to stop the autoimmune process that destroys the pancreas.
Co-morbidities. Autoimmune diseases such as celiac disease
& autoimmune thyroiditis are associated with type 1
diabetes.
Type 2 Diabetes
The first stage in the development of type 2 diabetes
is often insulin resistance causing an inadequate response
to insulin & requiring increasing amounts of insulin to control blood glucose.
Initially, the pancreas responds by producing more insulin, but after several years, insulin production may decrease
& diabetes develops.
Type 2 diabetes used to occur mainly in adults who
were overweight & ages 40 & older. Now, as more
children & adolescents in the United States become overweight & inactive, type 2 diabetes is occurring more often in young people.
Type 2 diabetes is more common in certain racial & ethnic groups such as African Americans, American Indians, Hispanic/Latino Americans & some Asian & Pacific Islander Americans. The increased
incidence of type 2 diabetes in youth is a “first
consequence” of the obesity epidemic among young people, a significant & growing public health problem.
Overweight children are at increased
risk for developing type 2 diabetes during
childhood, adolescence & later in life.
Symptoms. Type
2 diabetes usually develops slowly & insidiously in children. Symptoms may be similar to those of type 1 diabetes. A child or teen can feel very tired, thirsty, or nauseated & have to urinate often.
Other symptoms may include weight loss, blurred vision,
frequent infections & slow healing of wounds or sores.
Some children or adolescents with type 2 diabetes may show
no symptoms at all when they're diagnosed & others may present
with vaginal yeast infection or burning on urination due to yeast infection.
Therefore, it's important for health care providers to identify & test children or teens who are at high risk for the disease.
Signs of Diabetes. Physical signs of insulin resistance include acanthosis nigricans, where the skin around the neck or in the armpits appears dark, thick & feels velvety.
High blood pressure & dyslipidemia also are associated with insulin resistance.
Risk Factors. Being
overweight, having a family member who has type 2 diabetes, being a member of a high risk ethnic group, having signs of insulin resistance, being older than 10 years of age & experiencing puberty are risk factors for the disease.
Co-morbidities. Children with type 2 diabetes also are at risk for the long-term complications of diabetes & the co-morbidities associated with insulin resistance (lipid abnormalities & hypertension).
The cornerstone of diabetes management for children
with type 2 is healthy eating, with portion control &
increased physical activity. To control their diabetes, children with type 2 diabetes also may need to take oral anti-diabetes medication, insulin, or both.
Ongoing efforts to prevent & treat type 2 diabetes in children will require the involvement of health care
providers, school personnel, community institutions &
government agencies working together.
Gestational Diabetes
Gestational
diabetes mellitus (GDM) is a form of diabetes that's diagnosed in about 7% of all pregnancies, at a rate of about 200,000 per year. It's more common among obese women, women with a family history of diabetes &
among African American, Hispanic/Latino American & American
Indian women.
During pregnancy,
GDM must be treated to normalize maternal blood glucose
levels & avoid complications in the infant.
GDM imparts a lifetime
risk for type 2 diabetes although the risk is highest 5 to 10 years after delivery. In women with a history of GDM, even 10 years postpartum,
the risk of developing diabetes is 70% higher than in a comparable group of women without GDM.
The children of
women with a history of GDM
also are at increased risk for obesity & diabetes compared to other children.
Overweight women
with a history of GDM can take steps to reduce their risk for diabetes
by losing at least 5 to 7% of their body weight & increasing
their physical activity.
The Diabetes Prevention
Program clinical trial & other studies have shown that type 2 diabetes can be delayed or prevented in women with a history
of GDM thru sustained weight loss & lifestyle changes & possibly, the use of medications.
Timely diagnosis & treatment
of type 2 diabetes, should
it develop despite efforts at prevention, can prevent or delay the onset of diabetes complications.(See "Resources" for information on gestational diabetes.)
“Hybrid” or “Mixed” Diabetes
While for the most part it's easy to determine if
a child or teenager has type 1 or type 2 diabetes, some
children have elements of both kinds of diabetes. This phenomenon may be called “hybrid” or “mixed”* diabetes.
It isn't surprising that some children have elements
of both type 1 and type 2 diabetes, given the fact that
more children are becoming overweight. Youth with “hybrid” diabetes are likely to have both:
- insulin resistance that's associated with obesity
& type 2 diabetes - antibodies against the pancreatic
islet cells that are associated with autoimmunity &
type 1 diabetes.
Signs &
symptoms. The signs & symptoms are the same as those for type 1 & type 2 diabetes.
Management.
At the time of diagnosis, the clinician should attempt to determine which type of diabetes is present. Measuring antibodies against islet cells and assessing insulin production by measuring C-peptide levels help make the distinction.
C-peptide levels are best determined about a year after diagnosis. The presence of hybrid diabetes may affect how the child or teen is treated. Insulin injections are likely to be needed
(as for type 1) & oral diabetes medications may be used
to improve insulin resistance (as for type 2).
It's important to counsel the child or teen about healthy eating habits & the need for daily physical activity so he or she can reach a healthy weight.
* Some people also may use the misleading term “double”
diabetes. Patients should be assured that this doesn't mean
that they have a greater risk for complications or “extra” disease compared to those with type 1 or type 2 diabetes.
Maturity-onset Diabetes
of the Young
Maturity-onset diabetes
of the young (MODY) is a rare form of diabetes in children that is caused by a single gene defect that results in faulty insulin secretion.
MODY is defined
by its early onset (usually before age 25), absence of ketosis & autosomal
dominant inheritance. Thus each child of a parent with MODY has a 50% chance of inheriting the same type of diabetes.
MODY is thought
to account for 2 to 5% of all cases of diabetes & often goes unrecognized.
Treatment of MODY
varies. Some children
respond to diet therapy, exercise &/or oral anti-diabetes medications that enhance insulin release. Others may require insulin therapy.
Secondary Diabetes
Diabetes can occur in children
with other diseases such as cystic fibrosis or those needing glucocorticoid
drugs. These causes may account for 1 to 5% of all diagnosed cases of diabetes.
Statistics
Diabetes is one
of the most common chronic diseases in school-aged children. In the United States, about 176,500 people under 20 years of age have diabetes.
About 1 in every
400 to 600 children, has type 1 diabetes.
Each year,
more than 13,000 children are diagnosed with type 1 diabetes.
The incidence of type 1 is about 7 per
100,000 per year in children ages 4 & under; 15 per 100,000 per year in children 5 to 9 years & about 22 per 100,000 per year in those 10 to14 years of age.
About 75% of all
newly diagnosed cases of type 1 diabetes occur in individuals younger than 18 years of age.
Currently, because
10 to 15% of children & teens are overweight – about double the number of 2 decades ago – increasing numbers of young people have type
2 diabetes.
In several clinic based studies, the percentage of children
with newly diagnosed diabetes classified as type 2 has
increased from less than 5% before 1994 to 30
to 50% in subsequent years.
Although no ethnic group is untouched by the problem, the disease disproportionately affects American Indian,
African American, Mexican American & Pacific
Islander youth.
An example of this overrepresentation is seen among Pima Indians where the prevalence of
type 2 diabetes among 15 to 19 year-olds is
5%.
According to the Centers for Disease Control &
Prevention (CDC), “at risk for overweight” is defined as being in the 85th to 94th percentile & “overweight” is defined
as at or above the 95th percentile on the
CDC’s Body Mass Index (BMI)-for-age growth charts.
These charts can be found at http://www.cdc.gov/nccdphp/dnpa/bmi/index.htm.
Identifying Children with Diabetes
The rate of beta cell destruction in type 1 diabetes
is quite variable--rapid in some individuals (mainly infants
& children) & slow in others (mainly adults). Children & adolescents may present with ketoacidosis as the first indication of the disease.
Others may have modest fasting hyperglycemia that rapidly changes to severe hyperglycemia &/or ketoacidosis in
the presence of infection or other stress.
Most children & adolescents diagnosed with type
2 diabetes are overweight or obese, insulin resistant, and
have a family history of type 2 diabetes. They also may have physical signs of insulin resistance such as acanthosis nigricans.
Diabetes complications such as microalbuminuria and
the presence of cardiovascular risk factors such as abnormal
cholesterol and high blood pressure have been
observed among teenage Pima Indians and in other pediatric populations in the United
States.
Undiagnosed type 2 diabetes in children and adolescents
may place these young people at early risk for cardiovascular
disease; however, no data are available to define the scope of this problem.
In adults, up to one-third of individuals who have type 2 diabetes are undiagnosed and at risk for microvascular and macrovascular complications of diabetes.
It's important, therefore, for health care providers to consider testing for diabetes in high risk or symptomatic children.
The American Academy of Pediatrics & the American
Diabetes Association have developed the following testing
criteria and diabetes risk factors that health care providers can use to help identify type 2 diabetes in children before the onset of complications.
Testing Criteria
1. Overweight or at risk for overweight, defined
as BMI > 85th percentile for age & sex; weight for
height >85th percentile; or weight >120 % of ideal for height PLUS
2. Any two of the following risk factors:
Family history of type 2 diabetes in first- or second-degree
relative American Indian, African American, Hispanic/Latino,
Asian American, or Pacific Islander heritage
Signs of insulin resistance or conditions associated
with insulin resistance (acanthosis nigricans, hypertension,
dyslipidemia, polycystic ovarian syndrome)
Age to begin testing--10 years old or at onset of puberty if puberty occurs earlier
Frequency of testing--every 2 years
Test to use--fasting plasma glucose
Treatment Strategies
The basic elements of type 1 diabetes management
are insulin administration, nutrition management, physical
activity, blood glucose testing, and the avoidance of hypoglycemia. Algorithms are used for insulin dosing based on blood glucose level and food intake.
Children receiving fixed insulin doses of intermediate-
and rapid-acting insulins must have food given at the time
of peak action of the insulin. Children receiving a long-acting insulin analogue or using an insulin pump receive a rapid-acting insulin analogue just before a meal, with the amount of pre-meal
insulin based on carbohydrate content of the meal using
an insulin:carbohydrate ratio and a sliding scale for hyperglycemia.
Further adjustment of insulin or food intake may
be made based on anticipation of special circumstances such
as increased exercise. Children on these regimens are expected
to check their blood glucose levels routinely before meals and at bedtime.
Management of type 2 diabetes involves nutrition
management, increased physical activity, and blood glucose
testing. If this is not sufficient to normalize blood glucose levels, oral anti-diabetes medication and/or insulin therapy are used as well. The only oral agent approved for use in children
and adolescents is metformin.
All aspects of the regimen are individualized. (See Tip Sheets
for Kids with Type 2 Diabetes)
There is no single recipe to manage diabetes that
fits all children. Blood glucose targets, frequency of blood
glucose testing, type, dose and frequency of insulin, use of insulin injections or a pump, and details of nutrition management, all may vary among individuals.
The family and diabetes care team determine the regimen that best suits each child’s individual characteristics and circumstances.
Blood Glucose Goals
To control diabetes and prevent complications, blood
glucose levels must be managed as close to a "normal" range
as is safely possible (70 to 100 mg/dl before eating). Families should work with their health care team to set target blood glucose levels appropriate for the child.
The American Diabetes Association has developed recommendations
for blood glucose goals for young people with type 1 diabetes.
Although there are no national recommendations for children with type 2 diabetes, it may be reasonable to use the values in the following table as a guide.
Optimal plasma blood glucose and A1C
goals for type 1 diabetes by age group are:
Plasma Blood Glucose Goal
Range (mg/dl)
Values by Age
(Years) Before
Meals Bedtime/Overnight
A1C
Percent Rationale
Toddlers & preschoolers under age 6 100–180 110–200 <8.5 but
>7.5
• High risk and vulnerability to hypoglycemia
School age, ages 6 to 12 90–180 100–180 <8
• Risks of hypoglycemia and relatively low risk of complications
prior to puberty
Adolescents and 90–130 90–150
<7.5*
• Risk of hypoglycemia young adults, ages 13 to 19
• Developmental and psychological issues
Key concepts in setting glycemic goals:
• Goals should be individualized and lower
goals may be reasonable based on benefit: risk assessment.
• Blood glucose goals should be higher than
those listed above in children with frequent hypoglycemia
or hypoglycemia unawareness.
• Postprandial blood glucose values should
be measured when there is a disparity between preprandial
blood glucose values and A1C levels.
* A lower goal (<7.0)
is reasonable if it can be achieved without excessive hypoglycemia.
Hypoglycemia
Diabetes treatment can sometimes cause blood glucose
levels to drop too low, with resultant hypoglycemia.
Taking too much insulin, missing a meal or snack,
or exercising too much may cause hypoglycemia. A child can
become irritable, shaky, and confused. When blood glucose levels fall very low, loss of consciousness or seizures may develop.
When hypoglycemia is recognized, the child should
drink or eat a concentrated sugar to raise the blood glucose
value to greater than 80 mg/dl.
Once the blood glucose is over 80, the child can
eat food containing protein to maintain blood glucose levels
in the normal range. The concentrated sugar will increase
blood glucose levels and cause resolution of symptoms quickly, avoiding over-treatment of “lows.” If the child is unable to eat or drink, a glucose gel may be administered to the
buccal mucosa of the cheek or glucagon may be injected.
Glycemic goals may need to be modified to take into
account the fact that most children younger than 6 or 7
years of age have a form of "hypoglycemic unawareness." They lack the cognitive capacity to recognize and respond to hypoglycemic symptoms and may be at greater risk for hypoglycemia.16
Hyperglycemia
Causes of hyperglycemia include forgetting to take
medications on time, eating too much, and getting too little
exercise. Being ill also can raise blood glucose levels. Over time, hyperglycemia can cause damage to the eyes, kidneys, nerves, blood vessels, gums, and teeth.
Intercurrent illnesses are more frequent in young
children. Sick-day management rules, including assessment
for ketosis with every illness, must be established for children with type 1 diabetes.
Families need to be taught what to do for vomiting
and for ketosis to prevent severe hyperglycemia and
ketoacidosis.17
Monitoring Complications and Reducing CVD Risk
The following recommendations are based on the American
Diabetes Association’s standards of Medical
Care.16
Retinopathy. Although retinopathy most commonly occurs after the onset of puberty
and after 5–10 years of diabetes duration, it has
been reported in prepubertal children and with diabetes duration of only 1–2 years. Referrals should be made to eye care professionals with expertise in diabetic retinopathy, an understanding of the risk for retinopathy in the pediatric population, as well as experience in counseling the pediatric patient and family on the importance
of early prevention/intervention.
The first ophthalmologic examination should be obtained
once the child is 10 years of age or older and has had diabetes
for 3–5 years. After the initial examination, annual routine follow-up is generally recommended. Less frequent examinations may be acceptable on the advice of an eye care professional.
Nephropathy. To reduce the risk and/or slow the progression of nephropathy, optimize glucose and blood pressure control. Annual screening for microalbuminuria should be initiated once the child is 10
years of age and has had diabetes for 5 years. Screening
may be done with a random spot urine sample analyzed for
microalbumin-to-creatinine ratio. Confirmed, persistently elevated microalbumin levels should be treated with an ACE inhibitor, titrated to normalization of microalbumin excretion if
possible.
Neuropathy. Although it is unclear whether foot examinations are important in children and adolescents, annual foot examinations are painless, inexpensive, and provide an opportunity for education about foot care. The risk for foot complications is increased
in people who have had diabetes over 10 years.
Lipids. In children older than 2 years of age with a family history of total cholesterol over 240 mg/dl, or a CVD event before age 55, or if family history is unknown, perform
a lipid profile after diagnosis of diabetes and when glucose
control has been established. If family history is not a concern, then perform a lipid profile at puberty. Based on data obtained from studies in adults, having diabetes is equivalent to having had a heart attack, making diabetes a key risk factor
for future cardiovascular disease.
Pubertal children should have a lipid profile at
the time of diagnosis after glucose control has been established.
If lipid values fall within the accepted risk levels (LDL less than 100 mg/dl), repeat lipid profile every 5 years.
The goal for LDL-cholesterol in children and adolescents
with diabetes is less than 100 mg/dl (2.60 mmol/l). If the
LDL-cholesterol is greater than 100 mg/dl, the child should be treated with an exercise plan and a Step 2 American Heart Association diet. If, after 6 months of diet and exercise,
the LDL-C level remains above 160 mg/dl, pharmacologic agents
should be given. If, the LDL-C is between 130 and 160 mg/dl,
pharmacologic therapy should be considered. Statins are the agents of choice. Weight loss, increased physical activity, and improvement in glycemic control often result in improvements in lipid levels.
Blood pressure. Careful control of hypertension in children is critical. Hypertension
in childhood is defined as an average systolic
or diastolic blood pressure >95th percentile for age, sex, and height measured on at least three separate days. Normal blood pressure levels
for age, sex, and height, appropriate methods for measurement,
and treatment recommendations are available online at: www.nhlbi.nih.gov/health/prof/heart/hbp/hbp_ped.pdf.19
ACE inhibitors are the agents of choice in children
with microalbuminuria. They have beneficial effects on slowing
progression or preventing diabetic nephropathy.
Visiting the Health Care Team
Because most newly diagnosed cases of type 1 diabetes
occur in individuals younger than 18 years of age, and more
children and teens are now getting type 2 diabetes, care of this group requires integration of diabetes management with the complicated physical and emotional growth needs of children, adolescents, and their families, as well as with their emerging
autonomy and independence.
Diabetes care for children should be provided by
a team that can deal with these special medical, educational,
nutritional, and behavioral issues. The team usually consists of a physician, diabetes educator, dietitian, social worker or psychologist, along with the patient and family.
Children should be seen by the team at diagnosis and in follow-up, as agreed upon by the primary care provider and the diabetes team. The following schedule of care is based on the American
Diabetes Association’s Standards of Medical
Care, published in 2005.16
At Diagnosis:
• Establish
the goals of care and required treatment.
• Check lipids
in children with a significant family history*
• Begin diabetes
self-management education about healthy eating habits, daily physical activity, and insulin/medication administration, and self-monitoring of blood glucose levels if appropriate. A solid educational base is needed so that the individual and family can become increasingly independent in self-management of diabetes. Diabetes educators play an important role in this aspect of management.
• Provide nutritional
therapy by an individual experienced with the nutritional needs of the growing child and the behavioral issues that have an impact on adolescent diets.
• Conduct a
psychosocial assessment to identify emotional and behavioral disorders.
* In children with no significant family history, check lipids at puberty and if normal, repeat profile
every 5 years (see section on lipids for more information).
Each Quarterly Visit
Most young people with diabetes are seen by the health
care team every 3 months. At each visit, the following should
be monitored or examined:
• A1C, an indicator
of average blood glucose control
• Growth (height
and weight)
• BMI
• Blood pressure
• Injection
sites
• Self-testing
blood glucose records
• Psychosocial
assessment
Annually:
• Evaluate
nutrition therapy
• Provide ophthalmologic
examination (less often on the advice of an eye care professional)*
• Check for
microalbuminuria (once the child is 10 years old and has had diabetes for 5 years)
• Perform thyroid
function test (for children with type 1 diabetes)
• Administer
influenza vaccination
• Examine feet.
*The first ophthalmologic examination should be obtained
once the child is age 10 or older and has
had diabetes for 3 to 5 years.
Helping Children Manage Diabetes
The health care provider team, in partnership with
the young person with diabetes and caregivers, can develop
a personal diabetes plan for the child that puts a daily schedule in place to keep diabetes under control.
The plan shows the child how to follow a healthy
meal plan, get regular physical activity, check blood glucose
levels, take insulin or oral medication as prescribed, and manage hyperglycemia and hypoglycemia.
Follow a healthy meal
plan: Young people with diabetes need to follow a
meal plan developed by a registered dietitian, diabetes educator,
or physician. For children with type 1 diabetes, the meal plan must ensure proper nutrition for growth.
For children with type 2, the meal plan should outline
appropriate changes in eating habits that lead to better
energy balance and reduce or prevent obesity. A meal plan
also helps keep blood glucose levels in the target range.
Children or adolescents and their families can learn
how different types of food - especially carbohydrates such
as breads, pasta, and rice - can affect blood glucose levels. Portion sizes, the right amount of calories for the child's age, and ideas for healthy food choices at meal and snack time
also should be discussed including reduction in soda and
juice consumption.
Family support for following the meal plan and setting up regular meal times is a key to success, especially if the child
or teen is taking insulin. See NDEP’s
“Eat Healthy Foods” Tip Sheet for Kids with type 2 Diabetes.
For more information about healthy eating
for children, visit the American Dietetic Association, an NDEP partner. Their “Healthy Habits for Healthy Kids”
guide for parents is available in English and Spanish, and includes tips for a balanced diet. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) also offers diet tips for people
with diabetes.
Get regular physical activity: Children with diabetes need regular physical activity, ideally a total of 60 minutes each day. Physical
activity helps to lower blood glucose levels, especially
in children and adolescents with type 2 diabetes.
Physical activity is also a good way to help children
control their weight. In children with type 1 diabetes, the most common problem encountered during physical activity is hypoglycemia. If possible, a child or a teen should check blood glucose levels before
beginning a game or a sport. If blood glucose levels are
too low, the child should not be physically active until the low blood glucose level has been treated.
See NDEP’s “Be Active” Tip Sheet for Kids with type 2 Diabetes.
For more information on helping your child be physically
active, visit the Weight-Control Information Network (WIN)
of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). WIN offers a number of publications that address healthy eating
and physical activity. The Centers for Disease Control and Prevention’s (CDC) Verb campaign encourages youth to be physically active.
“Diabetes and Physical Activity at School”
provides additional information.
Check blood glucose levels regularly: Young people with diabetes should know the acceptable range for their
blood glucose. Children, particularly those using insulin
should check blood glucose values regularly with a blood glucose meter, preferably one with a built-in memory.
A health care team member can teach a child how to
use a blood glucose meter properly and how often to use
it. Children should keep a journal or other records of blood
glucose results to discuss with their health care team.
This information helps providers make any needed changes to the child's or teen's personal diabetes plan.
Take all diabetes medication
as prescribed: Parents, caregivers, school nurses, and others
can help a child or teen learn how to take medications as
prescribed.
For type
1 diabetes, a child or teen takes insulin at prescribed times each day via multiple injections or an insulin pump. Some young people with type 2 diabetes need oral medication or insulin or both.
In any case, it
is important to stress that all medication should be balanced with food and activity every day. “Managing Insulin Requirements at School” provides additional information.
Special Issues
Diabetes presents
unique issues for young people with the disease. Simple things, such as going to a birthday party, playing sports, or staying overnight with friends, need careful planning. Checking blood glucose, making correct food choices, and taking insulin or oral
medication can make school-age children feel "different"
from their classmates and this can be particularly bothersome for teens.
For any child or teen
with diabetes, learning to cope with the disease is a big task. Dealing with a chronic illness such as diabetes may
cause emotional and behavioral challenges, sometimes leading to depression. Talking to a social worker or psychologist may help young people and their families learn to adjust to the lifestyle changes needed to stay healthy.
Family Support
Managing diabetes
in children and adolescents is most effective when the entire family gets involved. Diabetes education should involve family members. Families can be encouraged to share concerns with physicians, diabetes educators, dietitians, and other health care
providers to get their help in the day-to-day management
of diabetes.
Extended family members,
teachers, school nurses, counselors, coaches, day care providers,
and other resources in the community can provide information, support, guidance, and help with coping skills. These individuals also may be knowledgeable about resources for health education, financial services, social services, mental health counseling, transportation,
and home visits.
Diabetes is stressful
for both the children and their families. Parents should be alert for signs of depression or eating disorders and seek appropriate treatment. While all parents should talk to their
children about avoiding tobacco, alcohol, and other drugs,
this is particularly important for children with diabetes.
Smoking & diabetes
each independently increase the risk of cardiovascular disease and people with diabetes who smoke have a greatly increased risk of heart disease and circulatory problems.
Binge drinking can cause hyperglycemia acutely, followed
by an increased risk of hypoglycemia. The symptoms of intoxication
are very similar to the symptoms of hypoglycemia & thus,
may result in delay of treatment of hypoglycemia with potentially disastrous consequences.
Transition to Independence
Children with diabetes
- depending on their age & level of maturity -will learn to take over much of their care. Most school-age children can recognize symptoms of hypoglycemia & monitor blood glucose levels.
They also participate in nutrition decisions. They
often can give their own insulin injections but may not
be able to draw up the dose accurately in a syringe until a developmental age of 11 to 12 years.
Adolescents often have the motor and cognitive skills
to perform all diabetes-related tasks and determine insulin
doses based on blood glucose levels and food intake. This is a time, however, when peer acceptance is important, risk-taking behaviors common & rebellion against authority is part
of teens’ search for independence.
Thus, adolescents must be supervised in their diabetes
tasks and allowed gradual independence with the understanding
that the independence will be continued only if they adhere
to the diabetes regimen and succeed in maintaining reasonable metabolic control.
During mid-adolescence, the family and health care team should stress to teens the importance of checking blood glucose levels prior to driving a car to avoid hypoglycemia while
driving.
Diabetes at School
The NDEP has developed a guide to educate & inform
school personnel about diabetes, how it's managed &
how each member of the school staff can help meet the needs of students with the disease.
School principals, administrators, nurses, teachers,
coaches, bus drivers, health care & lunchroom staff
all play a role in helping students with diabetes succeed.
Several Federal & some state laws provide protections
to children with disabilities, including diabetes. These
laws help ensure that all students with diabetes are educated in a medically safe environment & have the same access to educational opportunities as their peers - in public &
some private schools.
Students with diabetes are entitled to accommodations
& modifications necessary for them to stay healthy at
school.
Accommodations may need to be made in the classroom, with physical education, on field trips &/or for after-school
activities.
Written plans outlining each student’s diabetes
management help students, their families, school staff &
the student’s health care providers know what's expected of them.
These expectations should be laid out in written documents, such as:
-
Diabetes Medical Management Plan, developed by
the student’s personal health care team & family
-
Quick Reference Emergency Plan, which describes
how to recognize hypoglycemia & hyperglycemia &
what to do as soon as signs or symptoms of these conditions are observed
-
Education plans, such as the Section 504 Plan or
Individualized Education Program (IEP)
-
Care Plan or Individual Health Plan generated by
the school nurse that provides instructions to faculty &
staff.
The school nurse is the most appropriate person to
coordinate care for students with diabetes. Each student
with diabetes should have a written plan, developed by the school nurse, incorporating physician orders, parent requests & tailored to the specific developmental, physical, cognitive &
skill ability of the child.
The nurse will conduct a nursing assessment of the
student & develop a nursing care plan, taking into consideration
the child’s cognitive, emotional & physical status as well as the medical orders contained in the Diabetes Medical Management Plan.
A team approach to developing the care plan, involving the student, parent, health care provider, key school personnel & school nurse, is the most effective way to ensure safe and effective
diabetes management during the school day.
The nursing care plan would also identify school
employees assigned to provide care to an individual student,
under the direction of the school nurse, when allowed by state nurse practice acts. The school nurse is responsible for training, monitoring & supervising these school personnel.
The school nurse will promote & encourage independence & self-care consistent with the student’s
ability, skill, maturity & developmental level.
For more information on managing diabetes in the
school setting, see Helping the Student with Diabetes Succeed: A Guide for School Personnel.
Camps & Support Groups
Local peer groups &
camps for children & teens with diabetes can provide positive role models & group activities. Peer encouragement often helps children perform diabetes-related tasks that they'd been afraid to do previously & encourages independence in diabetes management.
Talking with other children who have diabetes
helps young people feel less isolated & less alone in having to deal with the demands of diabetes.
They have the opportunity
to discuss issues they share in common that others in their
peer group can’t understand & they can share solutions to problems that they've encountered.
Often, these programs
challenge children physically & teach them how to deal with increased exercise, reinforcing the fact that diabetes shouldn't limit them in their ability to perform strenuous physical activity.
Prevention Strategies for Type 2 Diabetes
For children & teens at risk, health care providers can encourage, support & educate the entire family to make lifestyle changes that may delay - or lower the risk for - the onset of type 2 diabetes.
Such lifestyle changes include keeping at a healthy weight & staying active. New research findings will
help determine effective ways to lower risk factors in high risk children. NDEP’s “Lower Your
Risk” Tip Sheet provides additional
information for children at risk of developing type 2 diabetes.
|
 |
|
It's in the news....
statistics
Total Prevalence of Diabetes in the United States, All Ages, 2005
Total: 20.8 million people -7% of the population -have diabetes.
Diagnosed: 14.6 million people
Undiagnosed: 6.2 million people
About 176,500 people aged 20 years or younger have diabetes.
This group represents 0.22% of all people in this age group.
About 1 in every 400 to 600 children & adolescents has type
1 diabetes.
Although type 2 diabetes can occur among youth, the nationally
representative data that would be needed to monitor diabetes trends in youth by type aren't available. Clinically based reports
& regional studies suggest that type 2 diabetes, although still rare, is being diagnosed more frequently in children &
adolescents, particularly in American Indians, African Americans & Hispanic/Latino Americans.
Total Prevalence of Diabetes Among People Aged 20 Years or
Older, United States, 2005
Age 20 years or older: 20.6 million; 9.6%
of all people in this age group have diabetes.
Age 60 years or older: 10.3 million; 20.9%
of all people in this age group have diabetes.
Men: 10.9 million; 10.5% of all men aged
20 years or older have diabetes.
Women: 9.7 million; 8.8% of all women aged
20 years or older have diabetes.
Total Prevalence of Diabetes
by Race/Ethnicity Among People Aged 20 Years or Older, United States, 2005
Non-Hispanic whites:
13.1 million; 8.7% of all non-Hispanic whites aged 20 years or older have diabetes.
Non-Hispanic
blacks: 3.2 million; 13.3% of all non-Hispanic blacks aged 20 years or older have diabetes.
After adjusting for population age differences, non-Hispanic blacks are 1.8 times as likely to have diabetes as non-Hispanic
whites of similar age.
Hispanic/Latino Americans:
After adjusting for population age differences, Mexican Americans, the largest Hispanic/Latino subgroup, are 1.7 times as
likely to have diabetes as non-Hispanic whites.
If the prevalence
of diabetes among Mexican Americans was applied to the total Hispanic/Latino population,
about 2.5 million (9.5%) Hispanic/Latino Americans aged 20 years or older would have diabetes.
Sufficient data
aren't available to derive estimates of the total prevalence of diabetes (both diagnosed & undiagnosed diabetes) for other Hispanic/Latino groups.
However, residents
of Puerto Rico are 1.8 times as likely to have diagnosed diabetes as non-Hispanic whites
in the United Sates.
American
Indians & Alaska Natives who receive care from the Indian Health Service (IHS): 99,500; 12.8% of American Indians
& Alaska Natives aged 20 years or older who received care from the Indian Health Service (IHS) in 2003 had diagnosed diabetes.
Applying the rate
of undiagnosed diabetes in the total U.S. population to the American Indians & Alaska
Natives who receive care from IHS gives an estimate of 118,000 (15.1%) American Indians & Alaska Natives aged 20
years or older with diabetes (both diagnosed & undiagnosed
diabetes).
After adjusting
for population age differences, the total prevalence of diabetes in this group is lowest
among Alaska Natives (8.1%) & highest among American Indians in the southern United States (26.7 %) & in southern
Arizona (27.6%).
Taking into account
population age differences, American Indians & Alaska Natives are 2.2 times as likely to have diabetes
as non-Hispanic whites.
Asian Americans
& Native Hawaiian or other Pacific Islanders: The total prevalence of diabetes
(both diagnosed & undiagnosed diabetes)
isn't available for Asian Americans or Pacific Islanders.
In Hawaii, however,
Asians, Native Hawaiians & other Pacific Islanders aged 20 years or older are more than 2 times as likely to have diagnosed
diabetes as whites after adjusting for population age differences.
Similarly in California,
Asians were 1.5 times as likely to have diagnosed diabetes as non-Hispanic whites. Other
groups within these populations also have increased risk for diabetes.
Deaths Among People with Diabetes, United States, 2002
- Diabetes was the 6th leading cause
of death listed on U.S. death certificates in 2002. This ranking is based on the 73,249 death certificates in which
diabetes was listed as the underlying cause of death. According to death certificate reports, diabetes contributed to a total
of 224,092 deaths.
- Diabetes is likely to be underreported as a cause of death.
Studies have found that only about 35 to 40% of decedents with diabetes have diabetes listed anywhere on the death certificate
& only about 10 to15% had it listed as the underlying cause of death.
- Overall, the risk for death among people with diabetes is about
twice that of people without diabetes of similar age.
Complications of Diabetes in the United States
Heart disease & stroke
- Heart disease & stroke account for about 65% of deaths in people with diabetes.
- Adults with diabetes have heart disease death rates about 2 to 4 times higher than adults without diabetes.
- The risk for stroke is 2 to 4 times higher among people with diabetes.
High blood pressure
- About 73% of adults with
diabetes have blood pressure greater than or equal to 130/80 mm Hg or use prescription medications
for hypertension.
Blindness
- Diabetes is the leading cause of
new cases of blindness among adults aged 20 to 74 years.
- Diabetic retinopathy causes
12,000 to 24,000 new cases of blindness each year.
Kidney disease
Nervous system disease
- About 60 to 70% of people with diabetes have mild to severe
forms of nervous system damage. The results of such damage include impaired sensation or pain in the feet or hands, slowed digestion of food in the stomach,
carpal tunnel syndrome & other nerve problems.
- Almost 30% of people with diabetes aged 40 years or older have impaired sensation in the feet (i.e., at least one area that
lacks feeling).
- Severe forms of diabetic nerve disease are a major contributing cause of lower-extremity amputations.
Amputations
- More than 60% of nontraumatic lower-limb
amputations occur among people with diabetes.
- In 2002, about 82,000 nontraumatic
lower-limb amputations were performed in people with diabetes.
Dental disease
- Periodontal (gum) disease
is more common in people with diabetes. Among young adults, those with diabetes have about twice the risk of those without
diabetes.
- Almost 1/3 of people with diabetes have severe periodontal diseases with loss of attachment of the gums to the teeth measuring 5 millimeters or more.
Complications of pregnancy
- Poorly controlled diabetes before conception & during the
first trimester of pregnancy can cause major birth defects in 5 to 10% of pregnancies &
spontaneous abortions in 15 to 20% of pregnancies.
- Poorly controlled diabetes during the 2nd & 3rd trimesters
of pregnancy can result in excessively large babies, posing a risk to both mother &
child.
Other complications
- Uncontrolled diabetes often leads to
biochemical imbalances that can cause acute life-threatening events, such as diabetic ketoacidosis & hyperosmolar
(nonketotic) coma.
- People with diabetes are more susceptible
to many other illnesses & once they acquire these illnesses, often have worse prognoses. i.e., they're more likely to die with pneumonia or influenza than people who don't have diabetes.
Prevention of Diabetes Complications
Diabetes can affect many parts
of the body & can lead to serious complications such as:
- blindness
- kidney damage
- lower-limb amputations
Working together, people with
diabetes & their health care providers can reduce the occurrence of these & other diabetes complications by controlling
the levels of:
- blood glucose
- blood pressure
- blood lipids
& by receiving other preventive care practices in a timely
manner.
Glucose control
- Studies in the United States & abroad have found that improved
glycemic control benefits people with either type 1 or type 2 diabetes.
In general, every percentage point drop in A1C blood test results
(e.g., from 8 to 7%) reduces the risk of microvascular complications (eye, kidney & nerve disease) is reduced by 40%
Blood pressure control
- Blood pressure control reduces the risk of cardiovascular disease
(heart disease or stroke) among persons with diabetes by 33 to 50 percent, and the risk of microvascular complications (eye,
kidney, and nerve disease) by about 33 percent.
- In general, for every 10 mm Hg reduction in systolic blood
pressure, the risk for any complication related to diabetes is reduced by 12%.
Control of blood lipids
- Improved control of cholesterol or blood lipids (i.e., HDL,
LDL & triglycerides) can reduce cardiovascular complications by 20 to 50%
Preventive care practices for eyes, kidneys & feet
- Detecting & treating diabetic eye disease with laser therapy
can reduce the development of severe vision loss by an estimated 50 to 60%
- Comprehensive foot care programs can reduce amputation rates
by 45 to 85%
- Detecting & treating early diabetic kidney disease by lowering
blood pressure can reduce the decline in kidney function by 30 to 70% Treatment with ACE inhibitors & angiotensin receptor
blockers (ARBs) are more effective in reducing the decline in kidney function than other blood pressure-lowering drugs.
NIH Publication No. 06–3892
November 2005
|
|
|
|
|
By Karla Gale
NEW YORK (Reuters Health)
- Heart disease, diabetes & depression can be a deadly combination, according results of a study that
suggest that, in people with coronary artery disease, the presence of diabetes or depression increases the risk of dying from heart disease.
The risk is even higher
when both diabetes & severe depression are present, investigators reported today at the annual meeting of the American Psychosomatic Society in Budapest, Hungary.
Dr. Lana L. Watkins &
her associates at Duke University in Durham, North Carolina studied 907 patients with coronary artery disease, which occurs when the arteries that supply blood to the heart muscle (coronary arteries)
become hardened & narrowed.
A total of 325 of the
patients also had type 2 diabetes. All of the study subjects were assessed for depression using a standard 21-item inventory.
During more than 4 years the
patients were followed, 135 patients died.
The researchers found that
depression & diabetes were both associated with increased death, independent of age, gender, body
weight & heart function.
Among diabetics
with coronary artery disease, having severe symptoms of depression further increased the risk by roughly 25%, the investigators report.
Researchers engineer stem cells to make insulin
Study using umbilical cord cells gives hope to future diabetes cure
May 25, 2007
WASHINGTON - Stem cells taken from the umbilical cords of newborns
can be engineered to produce insulin and may someday be used to treat diabetes, U.S. and British researchers reported on Friday.
They said they were able to first grow large numbers of the
stem cells and then direct them to resemble the insulin-producing cells of the pancreas that are damaged in diabetes.
“This discovery tells us that we have the potential to
produce insulin from adult stem cells to help people with diabetes,” said Dr. Randall Urban of the University of Texas
Medical Branch at Galveston, who directed the study.
“It doesn’t prove that we’re going to be able
to do this in people — it’s just the first step up the rung of the ladder,” Urban added in a statement.
Writing in the journal Cell Proliferation, the researchers,
who included a team at Britain’s University of Newcastle, said they hope to eventually produce an alternative to using
controversial embryonic stem cells.
In the United States, Congress has been fighting over whether
to increase federal funding of embryonic stem cell research, with opponents saying it is wrong to experiment on human embryos
and supporters saying the work is needed to transform many fields of medicine.
Regenerative medicine
Most of the science aims to create
a new field of regenerative medicine in which stem cells from a patient’s blood are grown and tweaked in the laboratory
and used to replace defective or damaged blood or tissue.
Other researchers are trying to learn how embryonic stem cells
give rise to all the tissues and parts of the body, while remaining virtually immortal themselves, in the hope of eventually
coaxing perhaps an ordinary skin cell to do the same.
The researchers in Texas and Newcastle used human umbilical
cord blood because it is an especially rich source of fresh “adult” stem cells.
One big hope is to create new pancreatic tissue for people with
diabetes. In type-1 diabetes, the body no longer produces insulin because those cells have been destroyed.
Stem cell expert Dr. Rudolf Jaenisch, of the Whitehead Institute
in Cambridge, Massachusetts, said he was skeptical about the research.
“In the past, these claims have been rather unconvincing,”
Jaenisch said in a telephone interview.
He said people who have tried to make insulin-producing
adult stem cells before have produced very small amounts of insulin, or have even been mistaken.
Last week, Geron Corp. said it had transformed human embryonic
stem cells into the pancreatic cells that produce insulin.
SARAH D. PRITTS, M.D., and JEFFREY SUSMAN, M.D.
University of Cincinnati College of Medicine, Cincinnati,
Ohio
Eating disorders, particularly anorexia nervosa & bulimia nervosa, are significant causes of morbidity & mortality among
adolescent females & young women.
Eating disorders are associated with devastating medical & psychologic consequences, including:
- death
- osteoporosis
- growth delay
- developmental delay
Prompt diagnosis is
linked to better outcomes. A good medical history is the most powerful tool. Simple screening questions, such as:
- "Do you think you should be dieting?"
can be integrated into routine visits.
Physical findings such
as:
- low body mass index
- amenorrhea
- bradycardia
- gastrointestinal disturbances
- skin changes
- changes in dentition
can help detect eating disorders.
Laboratory studies can
help diagnose these conditions & exclude underlying medical conditions. The family physician can play an important role
in diagnosing these illnesses & can coordinate the multidisciplinary team of psychiatrists, nutritionists & other
professionals to successfully treat patients with eating disorders. (Am Fam
Physician 2003;67:297-304,311-2. Copyright© 2003 American Academy of Family Physicians.)
Eating disorders are among the most common psychiatric problems that affect young women1 & these conditions impose a high burden
of morbidity & mortality.
Unfortunately,
the diagnosis of eating disorders can be elusive & more than 1/2 of all cases go undetected.2
The family physician's
office is an ideal setting to identify eating disorders & initiate treatment in a timely fashion. This review focuses on recognition & diagnosis of eating disorders in primary care.
A comprehensive review
of treatment & other aspects of these conditions is available in the American Psychiatric Association's practice guideline
on the treatment of eating disorders.3
Eating disorders occur most commonly in adolescents
and young adults and are 10 times more common in females than in males. They occur in all ethnic groups but are most common
among whites in industrialized nations. The principal eating disorders are anorexia nervosa, bulimia nervosa, and nonspecified
eating disorder. Anorexia has two subtypes--restricting type and binge-eating/purging type. Bulimia also has two subtypes--purging
and nonpurging.
In young women, the risk of developing anorexia
is 0.5 to 1 percent, and mortality is estimated at 4 to 10 percent.4,5 In the same population, the risk of developing
bulimia is 2 to 5 percent,1,6 and the incidence of disordered eating that does not meet strict criteria for eating
disorders may be twice that of the above conditions.2 Frequent dieting and desire for weight loss occur much more
commonly than overt eating disorders. In 1999, the Youth Risk Behavior Surveillance Survey7 reported that 58 percent
of students in the United States had exercised to lose weight, and 40 percent of students had restricted caloric intake in
an attempt to lose weight. Many adolescents and young adults who do not meet the strict diagnostic criteria for eating disorders
have disordered eating patterns, which can have a significant adverse impact on health. The distinction between normal dieting
and disordered eating is based on whether the patient has a distorted body image.
Risk factors for developing an eating
disorder include participation in activities that promote thinness, such as ballet dancing, modeling, and athletics,4
and certain personality traits, such as low self-esteem, difficulty expressing negative emotions, difficulty resolving conflict,
and being a perfectionist.1 Eating disorders are particularly common in young women with type 1 diabetes mellitus.
Up to one third of women with type 1 diabetes may have eating disorders, and these women are at especially high risk of microvascular
and metabolic complications.8
The role of family history in the
development of eating disorders is not clear. Some studies9 of twins demonstrate a strong link, and others demonstrate
no correlation. A family history of mood disorders in a first-degree relative also might be a risk factor.5
Early diagnosis with intervention and earlier age at diagnosis are correlated
with improved outcomes in patients who have eating disorders.5 Because family physicians serve as primary care
providers for a large percentage of adolescents, they have an important role in diagnosing these disorders.
The hallmark of anorexia is a refusal to maintain body weight at or above 85
percent of expected weight, as defined by age-appropriate body mass index charts. Patients with anorexia use caloric restriction
or excessive exercise to control emotional need or pain, and they are terrified of becoming overweight. Patients with nonpurging-type
bulimia also might severely restrict calories or exercise excessively to lose weight but do not meet the weight criteria for
diagnosis of anorexia.
Bulimia is characterized by uncontrollable binge-eating episodes, often followed
by purging behaviors such as vomiting or the use of laxatives. Patients with binge-eating/purging-type anorexia also might
binge and purge. Patients who have bulimia may be of normal weight, or they may be under- or overweight, whereas patients
with binge-eating/purging-type anorexia are underweight.
Diagnostic Criteria for Anorexia Nervosa
| A. |
Refusal to maintain body weight at or above
a minimally normal weight for age and height (e.g., weight loss leading to body weight less than 85 percent of that expected;
or failure to make expected weight gain during period of growth, leading to body weight less than 85 percent of that expected)
|
| B. |
Intense fear of gaining weight or becoming overweight,
even though patient is underweight |
| C. |
Disturbance in the way in which one's body weight
or shape is experienced, undue influence of body weight or shape on self-evaluation, or denial of the seriousness of the current
low body weight |
| D. |
Amenorrhea in postmenarchal females (i.e., the
absence of at least three consecutive menstrual cycles. A woman is considered to have amenorrhea if her periods occur only
following hormone administration.) |
Specify type:
Restricting type: during
the current episode, the patient has not regularly engaged in binge eating or purging (i.e., self-induced vomiting or the
misuse of laxatives, diuretics, or enemas)
Binge-eating/purging type:
during the current episode, the patient has regularly engaged in binge eating or purging
Reprinted with permission from Diagnostic and Statistical Manual of Mental Disorders. 4th ed, text
revision. Washington, D.C.: American Psychiatric Association, 2000:589.
Both of the major
eating disorders are characterized by a disturbance in the perception of body shape, which is closely tied to self-image.
Summaries of diagnostic
criteria for anorexia & bulimia are provided in Tables 1 & 2.10 It's also important to aggressively treat patients
who have traits of eating disorders but who don't meet the full criteria for anorexia or bulimia.11
Diagnostic Criteria for Bulimia Nervosa
Recurrent episodes
of binge eating. An episode of binge eating is characterized by both of the following:
A. In a discrete period of
time (e.g., within any 2 hr. period), eating an amount of food that is
larger than what most people would eat during a similar period of time & under similar circumstances
2. A sense of lack of control over eating during the episode
B. Recurrent inappropriate
compensatory behavior in order to prevent weight gain, such as self-induced vomiting; misuse of laxatives, diuretics, enemas,
or other medications; fasting; or exercising excessively
C. The binge eating & inappropriate compensatory behaviors both occur, on average, at least twice a week for 3 months
D. Self-evaluation is unduly influenced by body shape & weight
E. The disturbance doesn't occur exclusively during episodes of anorexia nervosa
Specify type:
Purging type:
during the current episode, the patient has regularly engaged in self-induced vomiting or the misuse of laxatives,
diuretics, or enemas
Nonpurging
type: during the current episode, the patient has used inappropriate compensatory behaviors, such as fasting or exercising
excessively, but hasn't regularly engaged in self-induced vomiting or the use of laxatives, diuretics, or enemas
Reprinted with permission from Diagnostic and Statistical Manual of Mental Disorders.
4th ed, text revision. Washington, D.C.: American Psychiatric Association, 2000:594.
Differential Diagnosis
A wide variety of medical problems can masquerade
as eating disorders. Hyperthyroidism, malignancy, inflammatory bowel disease, immunodeficiency, malabsorption, chronic infections,
Addison's disease, and diabetes should be considered before making a diagnosis of an eating disorder. Most patients with a
medical condition that leads to eating problems express concern over their weight loss. However, patients with an eating disorder
have a distorted body image and express a desire to be underweight.10
Psychiatric comorbidity is extremely
common; illnesses such as affective disorders, obsessive-compulsive disorder, somatization disorder, and substance abuse must
be considered when patients present with such symptoms.12
Major depression is the most common
comorbid condition among patients with anorexia, with a lifetime risk as high as 80 percent.5 Anxiety disorders,
especially social phobia, also are common.5 Obsessive-compulsive disorder has a prevalence of 30 percent among
patients with eating disorders.13 Substance abuse prevalence is estimated at 12 to 18 percent in patients with
anorexia and 30 to 70 percent in patients with bulimia.14
Personality disorders (Axis II diagnoses) also
are common, with comorbidity rates reported at 21 to 97 percent.15 The wide range is related to the complexity
of evaluating these diagnoses. Patients with bulimia are more likely to have a cluster B diagnosis (dramatic/ erratic), whereas
patients with anorexia are more likely to have a cluster C diagnosis (avoidant/anxious).15
Screening Tools
All patients in high-risk categories for eating
disorders should be screened during routine office visits.16 The medical history is the most powerful tool for
diagnosing eating disorders. Physical examination and laboratory findings might be normal, especially early in the course
of eating disorders.
A number of comprehensive psychiatric interviews
can be used to diagnose eating disorders,17,18 but these are impractical in the primary care setting. One promising
screening tool is the SCOFF questionnaire (Table 3).19 Because of its 12.5 percent false-positive
rate, this test is not sufficiently accurate for diagnosing eating disorders, but it is an appropriate screening tool.
SCOFF Questions
Do you make yourself Sick (induce vomiting) because you feel
uncomfortably full?
Do you worry that you have lost Control over how much you eat?
Have you recently lost more than One stone (14 lb [6.4 kg])
in a 3-month period?
Do you think you are too Fat, even though others say you are
too thin?
Would you say that Food dominates your life?
One point for every yes answer; a score >= 2 indicates a
likely case of anorexia nervosa or bulimia nervosa (sensitivity: 100%; specificity: 87.5%).
Reprinted with permission from Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: assessment of a new screening
tool for eating disorders. BMJ 1999; 319:1467.
Suggested Screening Questions for Anorexia Nervosa & Bulimia Nervosa
How many diets have you been on in the past year?
Do you think you should be dieting?
Are you dissatisfied with your body size?
Does your weight affect the way you think about yourself?
A positive response to any of these questions warrants further
evaluation.
Information from Anstine D, Grinenko D. Rapid screening for disordered eating in college-aged females in the primary
care setting. J Adolesc Health 2000;26:338-42.
Other screening questions that might be helpful
are listed in Table 4.18,20 Positive responses to any of these questions should prompt further
investigation with a more comprehensive questionnaire. When screening patients, it is important to take their developmental
stage into account; some questions might be inappropriate for younger patients.
History and Presenting Symptoms
Patients with eating disorders can have a wide
range of symptoms. Those with milder illness might have nonspecific complaints, such as fatigue, dizziness, or lack of energy.4
Patients might deny that they have symptoms, but their family members might express concern. Patients who have anorexia typically
will be unconcerned about significant weight loss. Other symptoms that might be reported or elicited include amenorrhea, sore
throat, gastroesophageal reflux disease, abdominal pain, cold intolerance, constipation, polyuria, polydipsia, and palpitations.
When taking a medical history, it is also important to take a dietary history to ask about the use of laxatives or diuretics.
Table 5 compares important clinical features of anorexia and bulimia.
see table 5 at the bottom of the page....
When obtaining a
history, it's important to establish trust & rapport with the patient, especially when the patient doesn't perceive
a problem. Talking to the family & patient together, as well as talking to the patient individually, is appropriate. If
the patient is an adolescent, questions must be asked in a developmentally appropriate, precise, nonjudgmental way.21
Physical Examination
Complications
of anorexia & bulimia can affect nearly every organ system. However, many patients might have a completely normal physical
examination, especially early in the disorder. It's important to explain to patients & their families that a normal physical
examination doesn't rule out an eating disorder.
Accurate weight measurements
are important in diagnosing an eating disorder. Abnormal growth curves, especially in children & adolescents, can be revealing. A patient who initially had normal growth
parameters might stop gaining weight or might lose weight while height increases. Eventually, height will be affected &
growth will diminish.
To obtain
accurate weight measurements, office staff must be trained to use standardized protocols to record consistent, reliable
measurements. Scales should be located in a private area & comments about weight should be minimized & made discreetly.
Staff should be aware that some patients with eating disorders, to avoid revealing their true weight, might drink extra fluids, put weights in their pockets, or wear layers of heavy clothing
before being weighed.1
Vital signs
might be abnormal, such as bradycardia, orthostatic hypotension & hypothermia. Abnormal skin findings include dry skin,
loss of subcutaneous fat, lanugo (fine body hair) & hypercarotenemia (an orange hue
caused by increased ingestion of carrots). Patients who induce vomiting might have calluses on the dorsum
of the dominant hand, as well as loss of dental enamel. Salivary gland enlargement is another sign of purging behavior.
Pulmonary complications
of eating disorders are rare, but vomiting can cause a pneumomediastinum. Pulmonary edema may occur in patients who undergo refeeding.
In addition
to bradycardia, cardiac findings may include acrocyanosis & decrease in overall heart size & stroke volume. Cardiomegaly
can indicate ipecac use. Electrocardiogram findings may include bradycardia, prolonged QT interval & nonspecific ST-T
changes.
The gastrointestinal
system also can be adversely affected. There can be decreased bowel motility, leading to abdominal distension. Gastroesophageal
reflux & pancreatitis can cause epigastric pain. If the patient is constipated, stool might be palpable in the left lower
quadrant.
Laboratory
Evaluation
Laboratory findings
might be completely normal, but targeted laboratory testing can be helpful to rule out medical illness. In patients who have
eating disorders, the complete blood cell count might be normal, but leukopenia isn't uncommon, probably because of increased margination
of neutrophils.
Immune
function doesn't appear to be impaired. In severe cases, pancytopenia might be present.12 Blood glucose
levels might be low.2 Hypochloremic, hypokalemic, or metabolic alkalosis might be present in patients who purge.
Hypokalemia
also might result from diuretic & laxative use. Severe hypokalemia might lead to cardiac arrhythmias, muscle weakness,
or confusion. Hyponatremia might occur with excessive water intake.
Thyroid-function
test findings might be consistent with the euthyroid sick syndrome, with low triiodothyronine & thyroxine levels
& a normal thyroid-stimulating hormone level.
Osteopenia
in eating disorders can result from several factors. Decreased estrogen levels & inadequate micronutrients, especially during adolescence
when bone strength is typically increasing, can lead to clinically significant osteopenia after as few as 6 months of illness.2
It's worthwhile to obtain dual-energy x-ray absorptiometry scans after 6 months of amenorrhea in patients with
anorexia & in patients with bulimia who have a history of anorexia.12
Treatment
Treatment
intensity & setting depend on the severity of the illness. Patients with mild illness can be managed on an outpatient
basis.
Patients
who are medically or psychiatrically unstable require inpatient treatment (Table 6).3 [Evidence
level C, expert opinion]
Treatment goals include attainment & maintenance of a healthy weight, management of physical complications, management of comorbid
psychiatric illness & prevention of relapse.
Eliciting
cooperation from the patient, helping to change maladaptive thoughts & educating the patient about proper health
& nutrition also are important.3
see table 6 below table 5 on the bottom of this page!
Adequate treatment of eating disorders requires
a multidisciplinary team approach. The family physician can and should be an integral member of that team. Early in the illness,
frequent visits to the primary care physician's office are helpful for surveillance of medical conditions, as well as for
nutritional re-education. The family physician also will be indispensable in the role of coordinating the entire team of professionals
involved in the patient's care.
Prognosis
The prognosis of patients who have eating disorders
is variable. The general consensus is that 50 percent of patients with anorexia have good outcomes, 30 percent have intermediate
outcomes, and 20 percent have poor outcomes. The percentages are similar in bulimic patients, with 45 percent having good
outcomes, 18 percent having intermediate outcomes, and 21 percent having poor outcomes. Patients with anorexia have a mortality
rate six times that of peers without anorexia.5
Factors that predict improved outcomes for eating
disorders include early age at diagnosis, brief interval before initiation of treatment, good parent-child relationships,
and having other healthy relationships with friends or therapists.5
Because of the severity of these illnesses and
the improvement in outcomes when diagnosis occurs earlier, the family physician can play a crucial role in helping patients
recover from eating disorders by detecting them at an early stage.
The authors indicate that they do not have any conflicts of interest. Sources of funding: none reported.
Members of various family practice departments develop articles for "Problem-Oriented Diagnosis." This is
one in a series from the Department of Family Medicine at the University of Cincinnati College of Medicine. Guest coordinator
of the series is Susan Montauk, M.D.
click here for source, authors & references
|
|
|
|
|
|
|
|